Hello, I'm Rebecca,
Founder of Neuroceptive Learning!
My Post-Traumatic Growth Story
My journey began in 2007 when, after a lifetime of being healthy and active, I suddenly experienced extreme pain, stiffness, weight gain, digestive problems, brain fog, and difficulty sleeping. After seeing many specialists, I was diagnosed with fibromyalgia and adrenal fatigue, which marked the start of my arduous journey to regain my health.
During this process, I faced many setbacks when trying to function at my previous level, which taught me the importance of listening to, being aware of my body, taking care of and regulating my health. Along the way, I had many AHA! Realisations that informed my being and service offerings at Neuroceptive Learning.

My first AHA! Realisation
“Health is not the absence of illness but rather our ability to feel safe, connect and regulate.”
In 2014, after stabilising my health and wanting to help others, I turned my experience into post-traumatic growth and started to retrain as a coach and therapist. I enrolled in coaching and biodynamic psychotherapy studies, focusing on body-oriented and somatic modalities. I aimed to explore methods that engage the whole person, not just their cognitive abilities, as many traditional top-down approaches do.
Through my Polarity studies, I encountered Stephen Porges' Polyvagal Theory, and I realised that my dysregulated Autonomic Nervous System (ANS) was causing my chronic fibromyalgia symptoms. The numerous dietary and detoxification protocols and awareness of what was happening in my body improved my Neuroception (my inner evaluation of safety), allowing my ANS to become more regulated.
It restored my physical health, as well as my relational and cognitive abilities, enabling me to experience psychological safety in my external world. I felt a sense of belonging and became more courageous in speaking up, contributing, and challenging within my family and the groups I belonged to.
“Polyvagal Theory is the science of feeling safe enough to fall in love with life and take the risks of living.”
— Deborah Dana, author of Anchored
My second AHA! Realisation
“Bottom Up - Sensory integration occurs before Neuroception & Cognition.”
Realising the importance of Neuroception, I became curious about how it can be influenced. With my Systemic and Computer Science background, I applied the principle of GIGO (Garbage In, Garbage Out) and the logical question was: what comes before Neuroception?
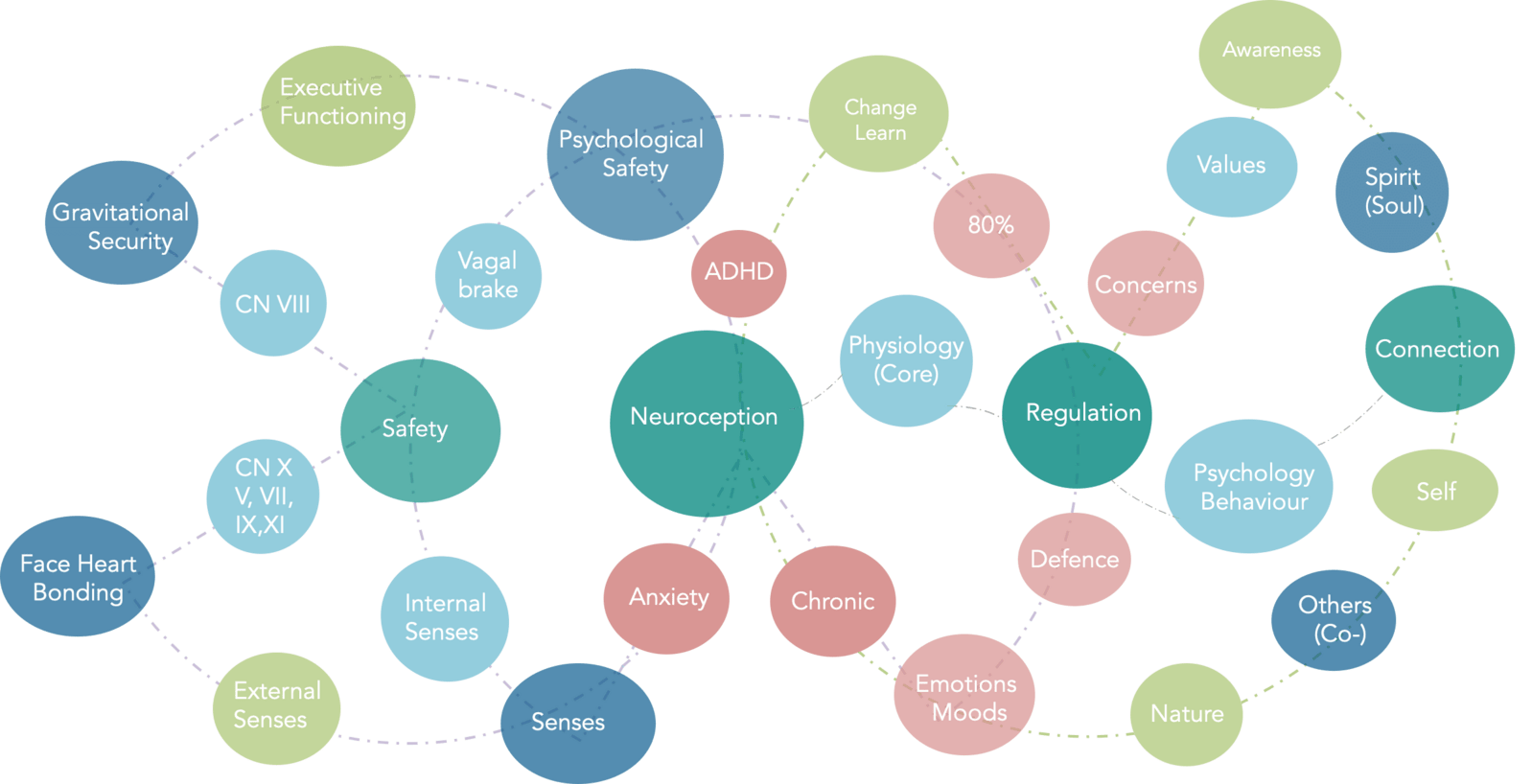
The inputs on which neuroception is based are multi-sensory integration and processing, gravitational security, face-heart-gut, face-heart, and vagal brake.
These are all part of our unique personal history, are embedded in our nervous system and are part of the sensory information from our internal bodies and external environment. Besides our five senses (touch, hearing, sight, taste and smell), we also have three internal senses: Interoception, Vestibular and Proprioception, which all provide sensory information mainly at our brainstem, where it is processed before neuroception, which activates our nervous system’s regulation and conscious cognition/thinking occurs.
While most current treatment interventions are top-down (from our thinking/cognition), combining them with approaches based on the natural way our nervous system functions: Bottom-Up.
This focus on our senses, the sensorimotor part of our nervous system, neuroplasticity and led to my third AHA! realisation:
“There is more wisdom in your body than in your deepest philosophy.”
— Nietzsche, Friedrich, Thus Spoke Zarathustra-
My third AHA! Realisation
“Our VUCA/BANI world resulted in dysregulated nervous systems.”
When I looked beyond my physical pain and digestive symptoms to my functional, behavioural and cognitive symptoms of sensory overload, sensitivity to light, smells, sound, touch, brain fog, procrastination and reactive responses - I saw similarities to those of the neurodiverse community, burn-out and other chronically ill individuals experienced. I realised that nervous system dysregulation has become the norm and manifests in many forms.
We live in a stress-filled zeitgeist, described as VUCA (Volatile, Uncertain, Chaotic, Anxious) or BANI (Brittle, Anxious, Non-linear, and incomprehensible). The WHO, ICD-11 in 2022, identified both Post-traumatic stress (PTSD) and Complex Post-traumatic stress (C-PTSD) as stress disorders of our time. Shock Trauma (PTSD) has been recognised since the 1980s, but we also now have ever-increasing conditions caused by chronic complex trauma/stress (C-PTSD), esp. relational and betrayal trauma. These results in compromised or dysregulated nervous systems, like mine was, for which one-off acute treatment solutions are insufficient. They require ongoing regulation approaches.
We cannot escape from our VUCA/BANI world. Still, we can learn how to support our nervous system’s regulation to experience psychological safety in our immediate environments.
Adverse Childhood experiences (ACEs) form a subset of C-PTSD, and because of the relational nature of C-PTSD, my studies took me to Psychosynthesis, Systemic and Family systems, and emerging Polyvagal informed neuro-somatic trauma modalities such as Somatic Experiencing, Neuro-affect relational model (NARM), Ego-states and Internal family systems.
This led to my 4th AHA! realisation of how we change.
"80 % of all illnesses have nervous system dysregulation as a root cause."
— James Jealous, osteopath and craniosacral trainer
My fourth AHA! realisation
Transformation through “intention/goal and will/motivation to change” and Beisser’s paradoxical theory of change: ”awareness of my present ontology.”
I realised that my desire and motivation for transformation/change had to come from within. I had to have the goal/intention of "wanting to heal" and the will and motivation to achieve that goal. But what ultimately brought about the change was when I became aware of my ontology: my way of being in life - in my doing, being, becoming, belonging and experience of psychological safety.
My ontology (survival adaptations or subpersonalities) influenced my way of being. ACEs led to the development of survival adaptive patterns or 'sub-personalities' that became embodied and rooted in my nervous system. These survival patterns are based on fear, and while they may have been helpful when they were first formed, they inhibited the expression of my true self/soul and intrinsic values. They also affect my motivation, will and reasons for wanting to change (my goal). Instead of being motivated by the intrinsic values of my soul purpose, my goals were based on the fears and concerns of the subpersonalities. Thus, they kept me in the past and prevented me from realising my full potential.
The more my ontology (way of being) in all its facets could be in my conscious awareness, the more choice, agency and self-leadership ultimately led to changes in my physical, behavioural and psychological health.
My ultimate AHA realisation was that …
“Health and wellness are not the absence of illness but rather our ability to feel safe, connect, regulate, and live according to the intrinsic values of our soul (soul values) in harmony with others and our environment.”
Neuroceptive Learning was Formed
I specifically chose “Neuroceptive Learning” because it encapsulates the essence of my healing journey and the services we provide.
The logo features a protea, the national flower of South Africa, my country of origin. The protea symbolises beauty, uniqueness, diversity, change, courage, and resilience. Like the protea, which thrives in harsh conditions, we must find psychological safety in a stressful VUCA/BANI world. We do this through neuroception (our inner evaluation/sense of safety).
Neuroceptive Learning uses different approaches to optimise our neuroception to support our nervous system regulation and, ultimately, our psychological safety in the external world. The goal is to promote self-leadership and facilitate change from within, radiating “psychological safety” to others in our immediate environment and, ultimately, the broader world.
Combining “OR” treatment solutions with “AND” regulation approaches to regain, maintain and generate ongoing health, well-being and happiness.
"Generating psychological safety in a VUCA/BANI world."
Degrees
- MA (Psychosynthesis Psychology) (Middlesex University)
- Post Graduate Diploma & Certificate in Coaching (University of Cambridge)
- MBA (University of Stellenbosch Business School)
- BCom Accountancy, Auditing (University of South Africa)
- BSc Computer Science, Mathematics (University of Stellenbosch)
Practitioner / Therapist
- Polarity
- Feldenkrais
- Sophrology
- Multi-Sensory Training Provider
- Somatic Experiencing
- Neuro Affect Relational Model (NARM)
- Continuum movement
- INPP Reflex Integration
- Blomberg Rhythmic Movements
- Kinflex
- Braingym and Touch for Health
- Tension and Trauma Release Exercises (TRE)
- Dr Ede Nutrition for Mental Health
- Wahl’s Nutritional protocol
- Insulin IQ Certified coach
- TRE Practitioner
- Insulin IQ Certified
- Scenar Facilitator
Coach, Trainer & Supervisor
- ICF professional & EMC Senior Coach
- ADHD Coach
- Psychosynthesis Leadership Coach
- Psychosynthesis Embodied Supervisor
- Solution Focused Coaching
- Ontological Coaching
- Leadership Embodiment
- mBraining & mBIT( Master)
- Systemic Constellations
Accreditation and Associations
- EMR
- ODAKT
- Polarity Verband Schweiz
- Feldenkrais Verband Schweiz
- ICF Professional Coach
- EMCC Senior Coach
- PACC (Professional Association of ADHD Coaches)
- EABP (European Association of Body Psychotherapy)
- International Sophrology Federation
- Agile Project & Change Management
- Point of Values
- Leadership Circle
- Leadership Embodiment
- Wahl’s Diet Protocol Practitioner
- Dr. Ede Ketogenic Diets for Mental Health
- Insulin-Smart Nutrition
- Fearless Organisations: Psychological Safety
- Polarity Management
- TRE Practioner
- Scenar Facilitator
Technology-Assisted Coaching Apps
- Unite Safe & Sound
- Heartmath
- Positive Intelligence
- Neurofit
Collaboration Partners
I have trained and collaborated with the following institutions: